


An Enigma: Transmission Of Epidemic Influenza (part 5)
I attempt to shed light on the riddle that is seasonal influenza using my bag of spanners. Today I take a look at crude mortality 1901 - 2022

I am now sitting on a pile of freshly-churned mortality data (influenza deaths per 100k population) differentiated by sex and age group that is capable of yielding no less than 18 separate charts for trends in mortality over a 122-year span. Whilst this is most excellent and a terribly yummy position to be in I’m going to risk the throwing of squishy tomatoes and rotten cabbages from readers and start with a plot of crude mortality for deaths ascribed to influenza. There is a jolly good reason for this that will manifest later, so bear with me.
Here is that potentially disappointing plot:
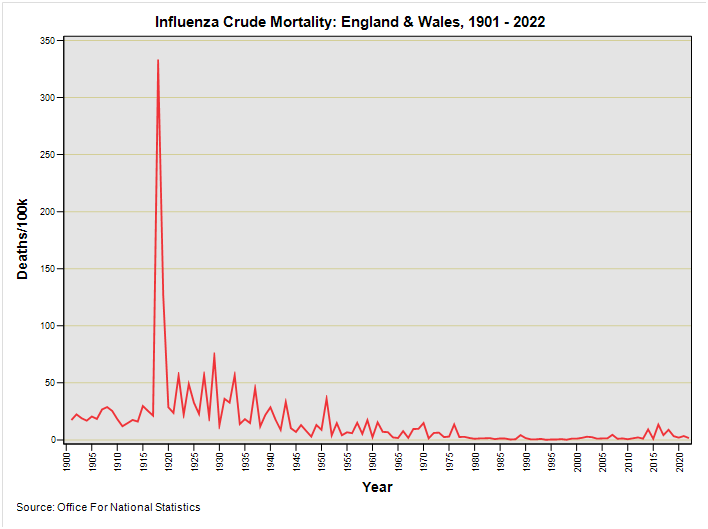
Those keen readers wot did their homework and went and read my five fabulous and utterly unctuous articles will be most familiar with this spiky slide. In eyeballing this variant we should note the lack of the pot holes arising from ONS experimentation with WHO Rule 3.
Because I’m a softie I’ll paste once again what I’ve already written about this bold swindling of cause of death coding…