COVID Uncovered (part 2)
Lessons from an undisclosed NHS Trust

In COVID Uncovered part 1 we took a look at admissions to the emergency department for a sizeable NHS Trust over the period Jan – Sep ’21 broken down by audited COVID status. We arrived at an audited status by considering all diagnoses made during triage along with presentation (a.k.a. chief complaint) and this enabled us to distinguish between asymptomatic COVID, mild COVID and various forms of severe COVID illness with or without significant comorbidities. Some 3,948 COVID admissions boiled down to just 129 cases that could be ascribed to severe COVID and severe COVID alone, this being a drop in the ocean of 296,331 admissions (0.04%). Folk are asking what the fuss was about. Quite.
This morning I thought I ought to apply the same diagnostic methodology to in-hospital deaths registered over the period Feb ‘20 – Sep ’21 for the same undisclosed Trust. In the first table below we observe a total of 20,987 deaths over the course of the pandemic, 83.6% of which were not associated with a positive PCR test…
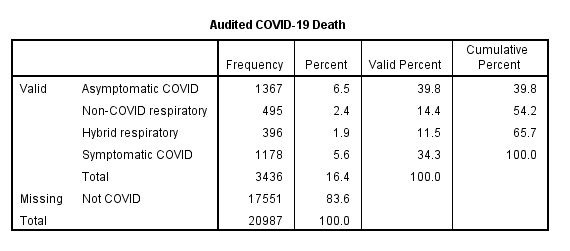
Of the remaining 3,436 positive-testing deaths we find 1,367 (39.8%) with absolutely no sign of any respiratory illness (asymptomatic cases). We also observe a further 495 deaths (14.4%) who died with a non-COVID respiratory condition (e.g. bacterial pneumonia), this bringing the total to 1,863 deaths (54.2%). At this point we may draw the sobering conclusion that the majority of COVID-positive deaths were not COVID causal - causal in the sense that COVID must lead to an acute respiratory condition rather than just a cough.
We find a further 396 COVID positive deaths categorised as ‘hybrid respiratory’ (11.5%). These are deaths where the cause is necessarily ambiguous in that both SARS-COV-2 and other pathogens such as staphylococcus could be equally be to blame for the onset of an acute respiratory condition. In this category I also included chronic conditions such as coalworker's pneumoconiosis, COPD, rheumatoid lung disease and tuberculosis. It would be medically erroneous to claim these as COVID only cases but that’s exactly how the Office for National Statistics (ONS) and its MUSE software go about things.
Finally, we get to the 1,178 deaths that we can confidently ascribe to symptomatic COVID (34.3%). These are cases exhibiting a cluster of acute respiratory symptoms for which no other respiratory/pulmonary cause was recorded. Though it would be tempting to automatically classify these as COVID-causal, we’ve another fence to jump and that is to consider major non-respiratory comorbidity that could also lead to death. An example here would be somebody testing positive with severe symptoms that lead to an acute respiratory condition but who dies from liver failure owing to the pharmacological load. Then there are those cases whose acute respiratory condition was successfully treated but who then go on to die from stroke, sepsis or multi-organ failure (for example in the case of late stage cancer). The ONS shovels all of these into the big pile they call COVID causal. Let us then squint at the second table…
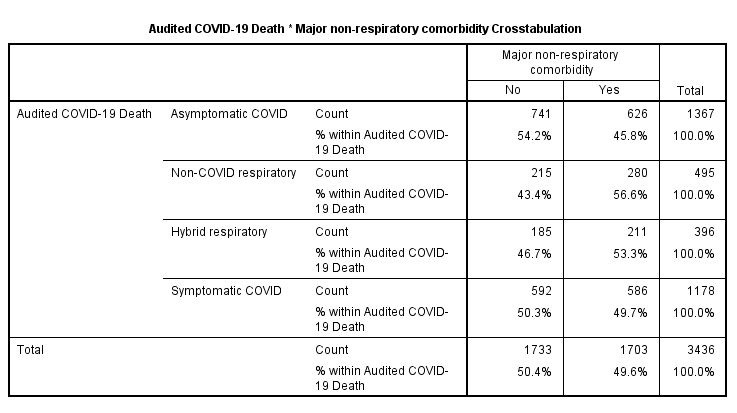
Well, now isn’t that interesting? Those 1,178 symptomatic COVID deaths just happen to be embracing 586 instances of major non-respiratory co-morbidity. This plonks us right into chicken-and-eggism where we cannot be sure which major morbidity was the actual cause of death and whether morbidities interacted. Clinicians will argue until the cows come home and not get to the bottom of such complex endpoints (I used to witness this monthly). Thus our sure-thing pile of bone fide COVID only causal deaths has been whittled down to 592 (17.2% of total COVID deaths).
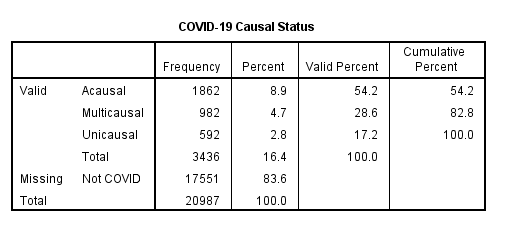
What we need now is to finish with a very simple table to sum causality in a tidy manner. Using table #2 I have concocted a crude causality indicator for positive-testing in-hospital death. This declares COVID deaths to be acausal (no respiratory condition), multicausal (more than one major morbidity potentially contributing to the cause of death) and unicausal (a COVID death that can be attributed solely to severe SARS-COV-2 infection). With just 17.2% of COVID deaths sitting under unicausal it is high time to get that kettle on methinks and allow clinicians to argue over those multicausal cases…