COVID Uncovered (part 3)
Lessons from an undisclosed NHS Trust

In parts 1 and 2 of this miniseries we discovered that severe SARS-COV-2 infection leading to development of COVID-19 symptoms, when viewed in terms of acute respiratory illness, hasn’t made much of an impression in terms of emergency department admissions or in-hospital deaths. Despite all the government propaganda COVID hasn’t been about people gasping for their last breath.
Back in March 2020 I would sit scratching my head over reports rolling in from clinicians week on week that were suggesting COVID was causing purple toes, bruising, skin rashes, diarrhoea, low blood pressure, vomiting, tachycardia, conjunctivitis, stroke, clotting, anorexia and even hair loss. This prompted a GP to wryly remark that he was going to blame his haemorrhoids on COVID. Were all these conditions – and many more to boot – genuinely a function of COVID (not forgetting long John COVID) or were they a function of reliance on an inappropriate diagnostic test?
With that bizarre medical episode at the back of my mind I set about this morning to see what 11,156 in-hospital deaths could tell us about COVID over the period 1st Feb – 7th December 2020 (i.e. the pandemic period prior to introduction of vaccines). Of those 11,156 deaths some 1,687 were classified as COVID deaths (15.1%), this number being just about sufficient to give some crude indication.
Being lazy I decided to avoid eyeballing several dozen tables and reached for staged multivariate logistic regression modelling instead. The idea here was to plonk incidence of COVID down as the dependent variable and let a whole host of independent variables jockey for position. I appreciate age and gender have a bearing, as well as overall health, so I opted to run these three explanatory variables plus their interactions though stage 1 to absorb basic variation in risk. ‘Overall health’ is impossible to judge from electronic records so I used the total number of diagnoses made per individual as a rough proxy. Not ideal but it’s the best I have!
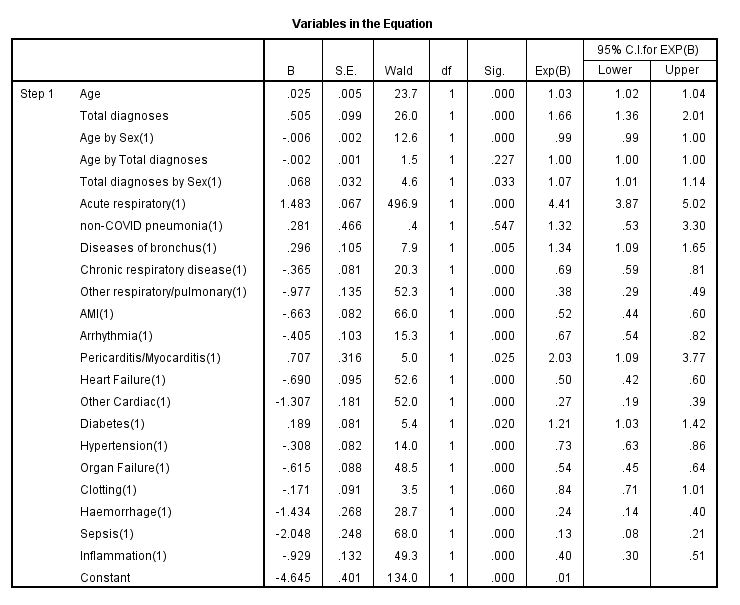
I’m not going to run through all the geeky detail and will just thrust this large table at folk for consideration. Key features to note are the strong positive association between COVID and acute respiratory conditions (OR=4.41, 95%CI[3.87;5.02], p<0.001), the positive association between COVID and diseases of the bronchus (OR=1.34, 95%CI[1.09;1.65], p=0.005), the positive association between COVID and pericarditis/myocarditis (OR=2.03, 95%CI[1.09;3.77],p=0.025), and the association between COVID and diabetes (OR=1.21, 95%CI[1.03;1.42], p=0.020).
Thus we see that COVID as an acute respiratory condition is pretty much where it’s at for those who go on to die, but what we also need to pay attention to here are pre-existing diseases of the bronchus that may be exacerbated, especially if these induce sepsis (and thus elevated risk of multi-organ failure). Interestingly, incidence of sepsis was strongly negatively correlated with COVID death (OR=0.13, 95%CI[0.08;0.21], p<0.001), along with organ failure (OR=0.54, 95%CI[0.45;0.64], p<0.001). Ideally clinicians would chew this over for us but what is clear is that nothing is clear, and we must take those case studies with a pinch of salt even when published in prestigious journals. I can hear our lead cardiac surgeon asking “so what were they doing wrong?” to which a colleague would respond, “so what are we getting right?”. Whatever the NHS Trust under study was doing between Feb and Dec 2020 sepsis and organ failure was not a feature of COVID death!
One little result that pleases me is that non-COVID pneumonia didn’t get tangled with COVID (p=0.547) - phew! One general feature of this table greatly intrigues me and this is the sheer number of diseases/conditions that are negatively correlated with incidence of COVID death in a statistically significant manner (12 out of a total of 17). This is most peculiar. We may conclude that COVID death was occurring in relatively healthy people (which is contrary to observation), or we may conclude something is amiss with the electronic patient record either in terms of completeness of record or accuracy of record. Then again we may question the validity of COVID designation. Something doesn’t stack up and I might need to invest in a decent tin of biscuits!