


Catastrophic Health Collapse (part 5)
In this article I utilise A&E admissions data for 2017 – 2021 from a sizeable NHS Trust to reveal trends in respiratory illness

In part 1 of this series I indicated I might publish extracts of some analytical work I have done using a rather useful dataset:
On a less subjective note I’ve also analysed emergency admissions and in-hospital death records for one of the UK’s largest NHS Trusts that confirm a substantial rise in respiratory illness prior to the alleged outbreak, with very little to show for the ‘pandemic’ year of 2020. I may well publish a summary of this work in a future article.
Back in late autumn of 2021 an anonymised data dump of emergency department admissions for a substantial NHS Trust for the period 2017/w1 – 2021/w37 was placed in my hands. I set about producing a series of reports so that healthcare professionals could chew over the fat rendered digestible by an independent soul who once did this sort of thing for a living in a busy teaching hospital. What I’m going to do today is reheat a batch of slides that reveal a flu-like illness smacked the UK a couple of months before HMG claimed COVID was a 'problem'.
Whilst it would be good to start with raw counts of admissions these figures don’t make that much sense given the extent of service closure so I’m going to offer slides for the percentage of respiratory admissions to all A&E admissions instead.
Wrinkle Cream
Before we get stuck in I ought to mention what is meant by a ‘respiratory admission’. Like all things in the medical world this is not the clear cut definition our minds would like to see. For example, somebody may be admitted to A&E with a broken leg but if they have asthma that condition may well be recorded also… or it may not. Whilst there’s a data capture system in place in reality a great deal of what eventually gets recorded depends on who is on duty, what the daily departmental workload is like and a few other things. A respiratory admission might well be somebody turning up because of a respiratory condition (a.k.a. chief complaint) but not necessarily so.
In terms of a chief complaint being banged into the older Accident and Emergency Commissioning Data Set (CDS type 010) that was used up until 2021 staff had three diagnostic choices for respiratory illness:
Respiratory conditions.
Respiratory conditions - bronchial asthma.
Respiratory conditions - other non-asthma.
Respiratory Profile 2017 – 2021
With all that in mind let us now consider two salient plots. What we’re doing here is swallowing the blue pill narrative by trying to fathom when we think SARS-COV-2 - an alleged respiratory pathogen - arrived on these shores and exploded in sufficient infectious number to swing the percentage of respiratory emergency admissions within a large NHS Trust. The green dashed line in the slide below marks 2020/w5 (w/e 31 January 2020), being the lull before the officially declared COVID storm.
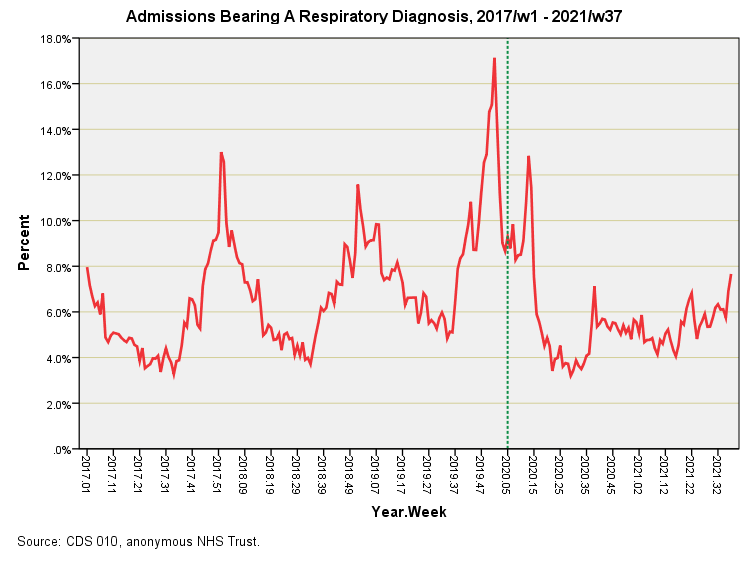
So when do we think a respiratory pathogen of some sort took hold of the fair nation of England? Yes indeed… it was in 2019.
November/December 2019 is the stand out period and that’s when most people I know went down with a flu-like illness with many saying it was the worst they’d experienced, me included. I’m betting good money on that December 2019 peak being a genuine pathogen that gave rise to what officials came to call COVID-19 once they had their hands on millions of test kits that would have ambiguously and most controversially ‘detected’ the nucleic acid aftermath. And so we find the respiratory horse had bolted before Boris had time to comb his hair and make his first big announcement in March 2020.
We may note the second peak at 2020/w13 (w/e 27 March 2020) that marks the beginning of the CHEC death spike period when the government decided to close the NHS down in a bid to save lives. Now that is some strange and most mysterious logic! It’s also worth asking how respiratory pathogens can strike twice within the space of 8 weeks, and I’m sure that digging deeper into the dataset will furnish an answer.
Here’s the profile for respiratory procedures undertaken in A&E:
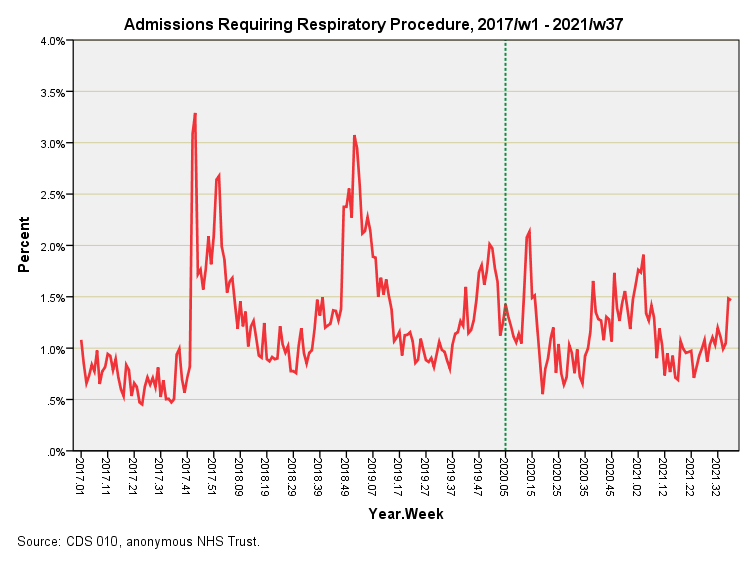
A respiratory procedure is defined as treatment with any of the following:
Chest drain
CPAP
Intubation/endotracheal tube
Lung punction
Nebuliser/spacer
Supplemental oxygen
Again we must note the real world wrinkles, for these procedures are not necessarily reserved for respiratory conditions only. Many will be used for those suffering a heart attack or suspected heart attack (precautionary), along with many and varied other conditions – traumatic chest injury, for example. Readers might spot use of supplemental oxygen and automatically think severe COVID. Not so! Oxygen is the most commonly used non-invasive therapy in use around the globe.
What we are looking at is rather interesting, with noteworthy surges back in 2017 and 2018. Modest use of these procedures during the December 2019 peak respiratory intake is fascinating, as is modest use during the alleged pandemic. There’s a blip that coincides with CHEC death spike period and we may wonder just what caused this. Does this mark the return of a respiratory pathogen within eight weeks or is it the hallmark of catastrophic policies, protocols and treatments?
Ideally we want to track use of respiratory procedures specifically for respiratory intake over this period to obtain a feel for the severity of situation. We can do this by deriving the ratio of respiratory procedures to respiratory diagnoses to provide what we might call a respiratory severity index (RSI). This is what the next slide offers:
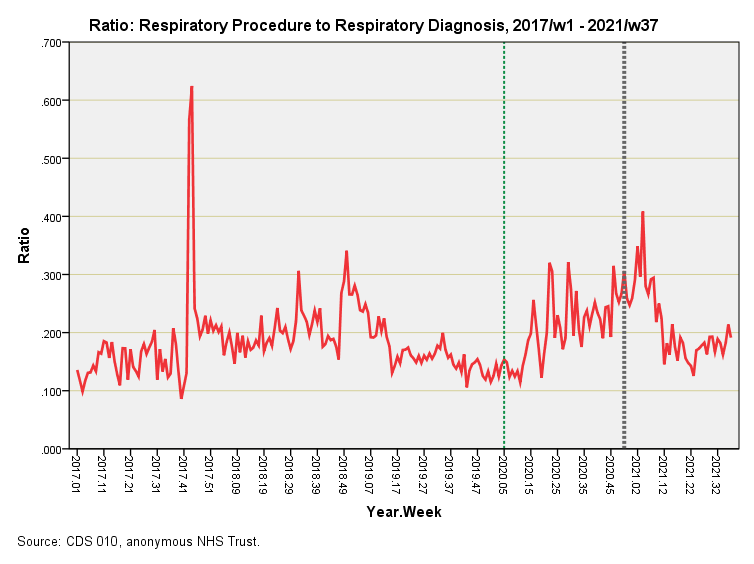
Something quite extraordinary happened back in 2017/w43 (w/e 27 October 2017) and 2017/w44 (w/e 3 November 2017) and we might jump to a conclusion involving a respiratory pathogen but this is not the only possibility. There remains the likelihood of a localised toxic spill or large building fire and there is even the possibility of a trial of new CPAP equipment. Please remember that very broad brushes are being used to paint these pictures, so treat outliers with caution!
The green dashed line in this plot again marks 2020/w5 (w/e 31 January 2020). What intrigues me is the extended quiet period during 2019 that indicates a lean year for respiratory pathogens, pollen counts, fungal spores and air pollution. Such a lean year builds the ‘tinderbox effect’ as stated previously.
We should note that the COVID era surge didn’t get going until 2020/w13, this being the beginning of the CHEC death spike period. Whilst we can clearly see a hump in RSI leading us through the 2020/21 seasonal peak for respiratory illness this bulge is not exceptional. An illusion is created by the unusually quiet year of 2019, and this can readily be seen if data for 2019 are covered by a slip of paper. When this is done the COVID era appears as a continuation of the historical trend in RSI. This is not the dynamic we may expect of an alleged novel and deadly virus: clearly it cannot have been either. If anything that spike for 2017/w43 – w44 was more like it!
The grey dashed line marks 2020/w50 (w/e 11 December 2020) this being the first week of vaccine rollout to the elderly and vulnerable whose number will already have been decimated during the CHEC death spike. That peak in the ratio occurring six weeks later is either evidence of delayed vaccine harm or evidence of a seasonal respiratory pathogen or both – a bit more digging is required.
I think it fair to say we’ve been conned, and not just by government spokespersons and their institutionalised experts but those in responsible positions in the NHS.
Kettle On!
Maybe the mysterious respiratory pathogen that returned within 8 weeks of the last one in early 2020 only existed in a model, was cloned and distributed? https://tessa.substack.com/p/jj-couey-virus-no-virus. But hey, "they" wouldn't do that, would they? And chemtrails is just another conspiracy theory...
Is it a possibility that the deaths in 2019 were people that had partaken a flu injection that season ? i.e. their immune system had been weakened ?