
Flip Flop Flu (part 1)
With the NHS straining under impressive levels of seasonal respiratory infection I decided to take a closer look at historical levels of death due to influenza and pneumonia

I’ve just sat down from gargling with aspirin. Whatever has been persistently raging through Mrs Dee’s school since September is now raging through the community at large. We’re talking colds, sore throats, snivels, hacking coughs, strep throat, fatigue, flu and being ‘hit by a bus’. Back in October the BBC asked: is the worst cold ever going round?
Being crusty around the edges I can recall worse winter seasons and being clobbered to point of being bed-ridden for two weeks, but here I am crunching numbers in my dressing gown and using the opportunity to sink hot toddies. Mrs Dee was clobbered with an upper respiratory tract infection for a couple of weeks back in October and we had thought my immune system had defended me successfully since nothing transpired upon my good self until the first week in December.
Plagued By The Plague
When it comes to considering transmission that sizeable delay from Dee to Dee is something I find rather intriguing – it took several weeks for me to finally succumb. Why? The same goes for other households hereabouts; then there’s the curious fact of many regions all being hit at the same time, and pretty much on a global basis.
The paradox of the perfect pandemic isn’t new news, being a curiosity that has plagued physicians for a couple of centuries:
Perhaps no disease has ever been observed to affect so many people in so short a time, as the Influenza, almost a whole city, town, or neighborhood becoming affected in a few days, indeed much sooner than could be supposed to spread from contagion. Mercatus relates, that when it prevailed in Spain, in 1557, the greatest part of the people were seized in one day. Dr. Glass says, when it was rife in Exeter, in 1729, two thousand were attacked in one night.
Shadrach Ricketson, M.D. (1808), A Brief History of the Influenza
The simple fact is to be recollected that this epidemic affects a whole region in the space of a week; nay, a whole continent as large as North America, together with all the West Indies, in the course of a few weeks, where the inhabitants over such vast extent of country, could not, within so short a lapse of a time, have had the least communication or intercourse whatever. This fact alone is sufficient to put all idea of its being propagated by contagion from one individual to another out of the question.
Alexander Jones, M.D. (1827), Philadelphia Journal of the Medical and Physical Sciences
… there are records of two other major epidemics of influenza in North America during the past two centuries. The first of these occurred in 1789, the year in which George Washington was inaugurated President. The first steamboat did not cross the Atlantic until 1819, and the first steam train did not run until 1830. Thus, this outbreak occurred when man's fastest conveyance was the galloping horse. Despite this fact, the influenza outbreak of 1789 spread with great rapidity; many times faster and many times farther than a horse could gallop.
James Bordley III, M.D. & A. McGehee Harvey, M.D. (1976), Two Centuries of American Medicine, 1776-1976
Why have epidemic patterns in Great Britain not altered in four centuries, centuries that have seen great increases in the speed of human transport?
John J. Cannell, M.D. (2008), On the Epidemiology of Influenza, in Virology
I recall the infamous ‘Hong Kong’ flu outbreak of 1968 rather well because I was rather ill, with the doctor being called to see me once per week. Despite my condition nobody else in my household was stricken and, in fact, nobody else in my extended family so much as snivelled despite this being labelled a contagious deadly disease arising from human-human transmission.
Hope In Hope-Simpson?
Perhaps we should take a closer look at the work of Hope-Simpson whose seminal (but rather expensive) The Transmission of Epidemic Influenza (Springer, 1992) embraces some rather controversial ideas. I’m not familiar with these so I have taken the liberty of ordering a copy and shall place the blame for such unwarranted expenditure on my febrile mind! I haven’t really tackled the paradoxical subject of SARS-COV-2 transmission as yet but shall run a series of articles once I get my brain around Hope-Simpson’s work on influenza.
Right now my gut feeling is that we’re not looking at transmission in terms of contagion (persons infecting persons) but a wave-like effect arising from the dissonance between internal (physiological) and external (environmental) conditions. I guess I’m thinking about flu in terms of a constant pathological pressure to which we individually succumb if conditions permit. If this hypothesis holds any water then it will certainly put the cat among the globalist gobble-gobble pigeons, especially those pushing lockdowns, masks, social distancing, quarantine camps and other forms of insidious non-pharmaceutical intervention.
I’m certainly not the only bod to question the official narrative of SARS-COV-2 as both a novel and a deadly virus that is transmitted from person to person, and in this regard I recommend Jonathan Engler’s articles on Northern Italy by way of a taster, which may be found here.
Oi, Let’s See Some Slides!
With the prologue ended and the scene set for our dramatical adventure into flu-flu-land I shall start by producing a slide of crude mortality (deaths per 100k population) for the period 1901 – 2021 for deaths due to influenza (ICD10 J09-J11) and pneumonia (ICD10 J12-J18) . This is based on an obscure dataset that some kind officer at the Office for National Statistics pointed in my general direction back in March 2021 (if anybody would like a copy please let me know):
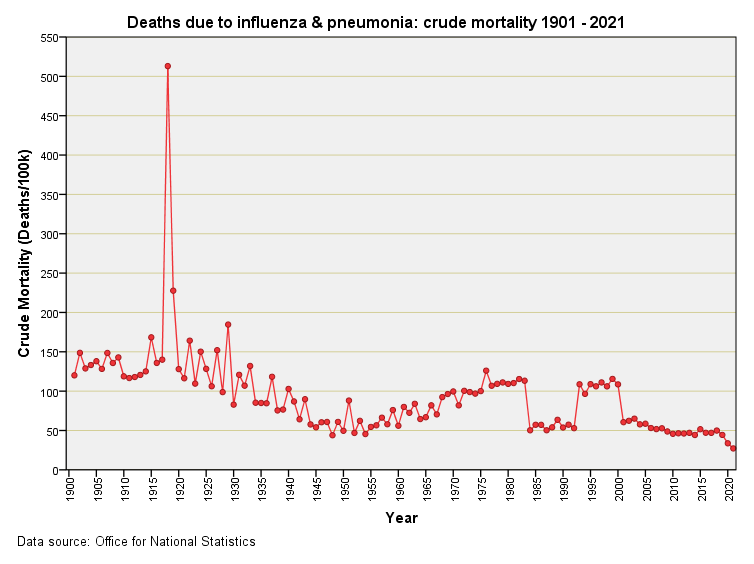
I think we can spot the pandemic of pandemics, being the Spanish Flu outbreak of 1918 – 1919!
We may note the gradual decline in crude mortality from that deadly moment in time onward down to a low that was reached during the 1950s. From 1955 onward things have steadily got worse and there will be folk who will want to point the finger of blame squarely at national vaccination programmes. Before we do this we need to figure population demographics, making adjustments for age, sex and occupation as well as accounting for trends such as smoking, environmental toxins, air pollution and the long term impact of WWII (manufacturing as well as conflict) to name but a few factors.
Coal mining, steel production and quarrying will have stored up respiratory trouble for the post-WWII populace, then there’s the impact of industries employing asbestos and other nasties. Apart from asbestos as a harbinger of respiratory illness we have coal dust, silica, talc, aluminium, bauxite, beryl, graphite, flax, mineral fibres, a variety of organic substances and a variety of inorganic substances. Then there’s mould, fungal spores and several bacterial strains that can induce pneumonia. Profession-wise we have farmer’s lung (ICD10 J670), maltworker’s lung (ICD10 J674), mushroom worker’s lung (ICD10 J675), and maple bark stripper’s lung (ICD10 J676),
Neither can we put the blame squarely on industry. Believe it or not there is such a thing as bird fancier’s lung (ICD10 J672) and air conditioning/de-humidifier lung (ICD10 J677).
If any of the aforementioned were on the rise after 1955 then we may expect to see an attendant rise in respiratory death. Attributing cause at the population level is fraught with difficulty because the list of confounding factors is usually astronomical; better then, to keep an open mind to all manner of possibility.
Jack In The Box
I hope at this juncture that everybody has seen the jack in the box that appears 1980 – 2005 or thereabouts. Respiratory death magically takes a dive during the period 1984 - 1992 only to emerge unscathed in 1993 before disappearing again forever in 2001. This weirdness is why I called this article ‘flip flop flu’.
After scratching around with bafflement on maximum I decided to write to the ONS and ask them for an explanation. An officer assured me that the data were indeed genuine and pointed me in the direction of documents that would explain everything. The culprit turned out to be a ruling by the World Health Organization known to ONS officers as ‘Rule 3’ - this rule changing all the rules for disease coding and classification.
I shall cover this fiddling in detail in the next article in this series but for now I want readers to realize that temporary rule changes for 1984 - 1992 that were made permanent back in 2001 have lead to lower estimates of crude mortality for influenza and pneumonia in recent years compared to historic levels. That is to say, a leading cause of death in these islands has been nobbled by bureaucrats wishing to de-emphasize the seriousness of respiratory illness.
If I was feeling cheeky I’d suggest that this was enacted to make flu vaccines look good, and to pave the way for the churning out of stats as evidential proof of record-breaking modern pandemics… but that may well be my febrile brain talking! Time for another hot toddy perhaps.
Kettle On!
Thanks for the mention, and sorry to hear you've been unwell - get better soon, we need you!!
Hope you feel better soon!