
Why The False Negative Argument Is False
Investigation of the hike in care home non-COVID deaths in England & Wales during 2020 (rev 2.3)

Subscribers following my newsletter series on care home deaths since 15th June will have surmised three things:
There was a dirty great hike in non-COVID care home deaths over the period 2020/w13 - 2020/w20 that synchronously occurred across all 10 regions at a time of year when this was not expected.
Hikes in non-COVID care home death precede hikes in COVID death by 1 - 2 weeks across all 10 regions in a consistent manner.
Peak COVID care home deaths during early 2020 occurred during the very same week across 9 regions, with the peak for London appearing just one week earlier. That is to say, there is no evidence of the SARS-COV-2 virus steadily spreading through the care home population.
Judging by comments received these are not just points of curiosity but highly disturbing in their implication. Before we go any further let me just pop this slide down that brings together the non-COVID and COVID death counts for England & Wales for the period 2020/w1 - 2022/w3:

We now see that non-COVID care home deaths out-gunned COVID deaths for all periods apart from 2021/w3 - 2021/w4, this being one jolly good reason why we should be bothered about them. We also observe just one moment in time when non-COVID death went through the roof one week ahead of COVID death. Whatever happened during 2020/w13 - 2020/w21 was never to repeat itself.
Some argue that this is all due to false negative test results. The problem I have with this is that we don’t see the issue arising again during the 2021 COVID peak, so these folk would also need to explain why the false negative issue magically disappeared from the care home scene. They’d also need to explain why that single and most substantial non-COVID peak occurred 1 - 2 weeks earlier, when theoretically it should peak at the same time. The sheer size of the numbers involved also cast a shadow on the false negative hypothesis.
Let Us Suppose…
Let us suppose all of those non-COVID deaths were false negatives. During 2020/w13 - 2020/w21 we find a total of 34,508 non-COVID and 17,194 COVID care home deaths across England & Wales within a total of 51,702 all cause deaths, which would push the false negative reporting rate to 67%. I think not!
Indeed not, for we can play with a handy calculator provided by the BMJ which may be found here (providing we have some sensible numbers to stick in). Experts at the ONS tell us that PCR test sensitivity is “somewhere between 85% and 98%”, with specificity quoted as “ very close to 100%”. Let us split the difference and go for a sensitivity of 92%, and use 99% for specificity, being the sensible types that we are. We now need a jolly decent estimate of disease prevalence (a.k.a. pre-test probability) for care homes in England & Wales. In a splendid IJE article which may be found here we find that “one in 20 long-term care facilities (LTCF) residents have been infected with COVID-19”; this gives us a pre-test probability of 5%. Turning the handle on the BMJ calculator I get this…
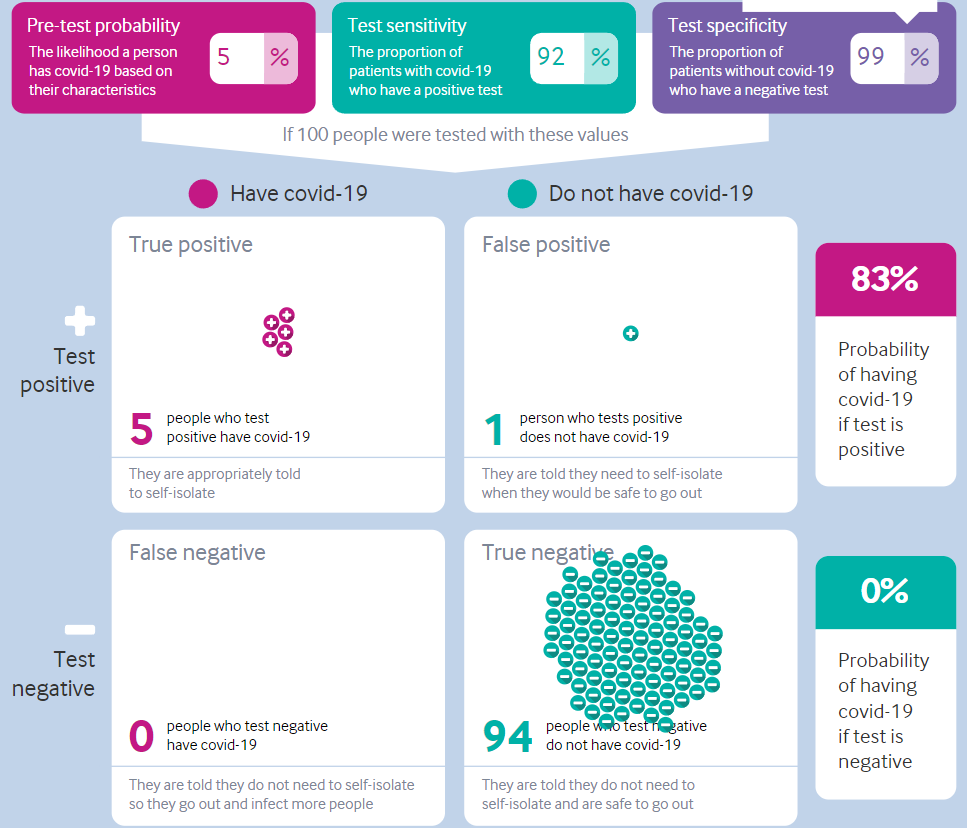
Does anybody see any false negatives cropping up at a rate of 67%, ‘cos I sure don’t!
La-La-Land
Let us now go to La-La-Land and assume a whopping great 50% pre-test probability (i.e. 1 in every 2 care home residents were infected with SARS-COV-2). I now get this scenario…
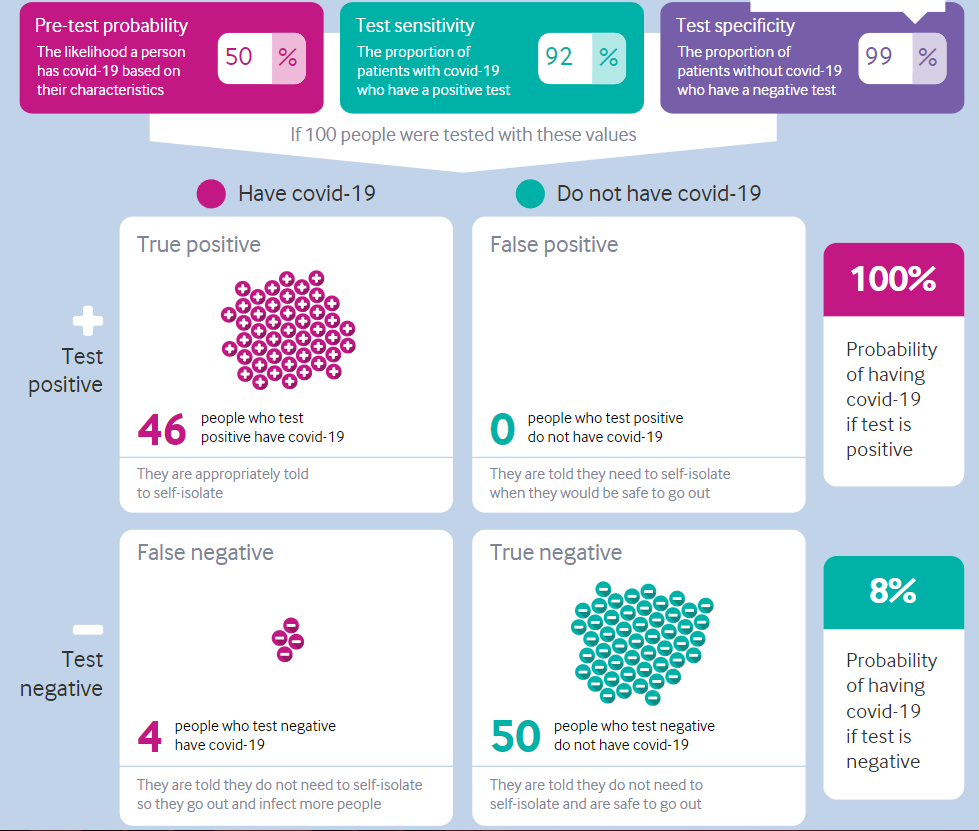
Does anybody see any false negatives cropping up at a rate of 67%, ‘cos I sure don’t! I get a lowly figure of 8% and that’s yer lot.
We may wonder at what level of pre-test probability will the false negative reporting rate hit 67% and the answer is a stonking great 96%. Nowhere in the literature can I find estimates of disease prevalence for any group of people anywhere near this. Over on UK GOV the findings from Imperial College London and Ipsos MORI, covering 8 March to 31 March 2022 (round 19 of the study), show “that prevalence in England during this period was 6.37%. This is the highest recorded figure since the beginning of the study in May 2020.” The same report also concludes that “the rate of prevalence among those who had been in contact with a positive case stood at 17.8% compared to 4.00% in those without such contact.”
It doesn’t take a genius to realise that 17.8% is a long way from 96%, and that even if the contact rate were higher for care home residents we’d still be a long way from 96%. We may conclude that the false negative argument for our care home big blip of death doesn’t cut the mustard, neither does it hold water (or anything else for that matter).
Let’s Be Sensible!
Up to this point I have argued in extremis; that is to say I have assumed every single one of the 34,508 non-COVID deaths must have been due to false negative test results. People still fall down the stairs and suffer from cardiac conditions so let us switch to the eminently sensible suggestion of assuming excess non-COVID deaths are where the problem lies. The figure of 11,253 was furnished in this newsletter of 17th June and this provides a false negative reporting rate of 22%. Now that’s more like it!
We may now ask what the pre-test probability should be in order to hit the magic 22% for false positive reporting and here’s the answer…
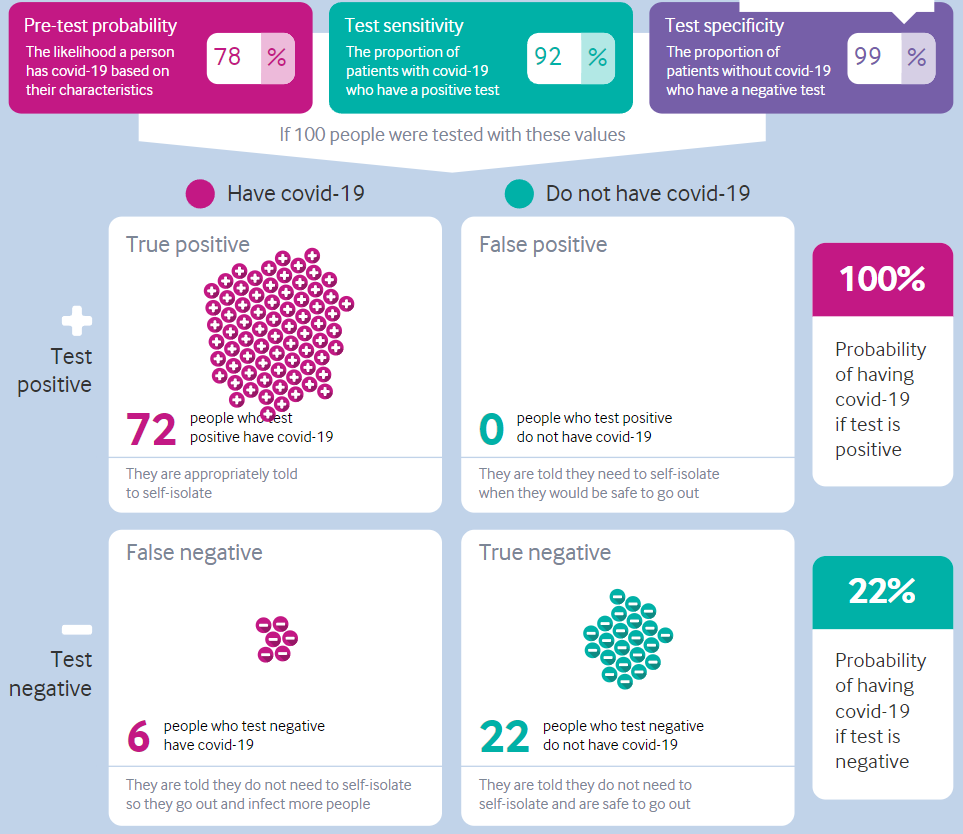
A pre-test probability of 78% may not be as crazy as 96% but it’s still pretty bonkers, yet this is our very best and most sensible guess!
So where does this leave us?
It means those arguing that false positive test results were likely responsible for the 11,253 excess non-COVID deaths in care homes across England & Wales over the period 2020/w13 - 2020/w21 are arguing that the pre-test probability (a.k.a disease prevalence) was as high as 78%; that is to say around 8 out of 10 care home residents were stricken with the infection. I don’t think so, thank you very much! These folk may not realise that this is what they are actually claiming but then again I’m pretty certain they haven’t bothered to sit down and figure the nitty gritty of PCR test performance.
A Fly In The Ointment
All this analysis assumes that care homes across England & Wales in early 2020 had access to PCR testing as and when required. Anecdotal evidence coming to me from those in the care sector suggests this was not the case. We must note that physicians could code COVID death merely by scribbling U07.2 COVID-19, virus unidentified on the death certificate. No test necessary! I trust physicians far more than I do the diagnostic test so we may ask why they opted to code these care home deaths as they did given they’d presumably be guided by symptom and clinical course. In this regard we must also note the buzzing in the ointment generated by WHO’s recommendations on death certification:
"With reference to section 4.2.3 of volume 2 of ICD-10, the purpose of mortality classification (coding) is to produce the most useful cause of death statistics possible. Thus, whether a sequence is listed as ‘rejected’ or ‘accepted’ may reflect interests of importance for public health rather than what is acceptable from a purely medical point of view. Therefore, always apply these instructions, whether they can be considered medically correct or not."
Bold is mine.
We are thus left with a hike in mortality that is being called COVID but may not be and a hike that is being called Non-COVID but may not be. Unless we get our hands on the medical notes accompanying each certificate we shall never know what happened back in early 2020. I shall end by suggesting that it is high time for a cuppa and a mid-morning biscuit or two.
Kettle On!
I have sometimes wondered if deaths were "encouraged" just long enough to get the ball rolling and bridge the gap to the start of the quasi-vaccination campaign.
I'm still baffled. The figures are very odd.
It might be worth exploring the history of 'fashionable' diseases...
Everyone was alerted about Covid, but anyway, what kind of hypotheses might be within the realm of possibility?
Could there have been an undetected strain of pneumonia, sepsis or some other background bug doing the rounds in Spring 2020, which then was confused with, masked by, and/or compounded the ill-effects of Covid-19?
Could we even be looking at the wrong pathogen altogether?
In the Lancet, at least one expert called this a 'Syndemic'... thats a clue. https://en.wikipedia.org/wiki/Syndemic
I mean, I've had Covid-19, probably twice, and really it isn't that bad. And I have zero medical or bacteriological qualifications. But maybe it was reacting with something else - a sort of double jeopardy? Or is this just a silly amateur idea?